Today we’d like to introduce you to Courtney Hunt.
Alright, so thank you so much for sharing your story and insight with our readers. To kick things off, can you tell us a bit about how you got started?
My grandmother’s journey fueled my desire to “do healthcare better” and become a nurse whom patients and families could trust. Fast forward to today: after 12 years in nursing and just days after my 35th birthday, my story took an unexpected pivot in the form of my grandfather’s unanticipated hospice journey.
Living in South Carolina for the past five years, I was often involved in Pop Pop’s care from a distance through regular phone reminders encouraging healthy eating and physical activity, fun FaceTime conversations, and surprise visits home for holidays and special occasions, including his 90th birthday. As the “nurse of the family,” my role in Pop Pop’s care became especially relevant at the end of his life, as I was tasked with being his hospice nurse while simultaneously guiding my family through the difficult and sensitive subject of death. Pop Pop would often make remarks about “being prepared for death” and “having your affairs in order,” but when that time was staring me in the face, the conversation around death looked and felt different as it unfolded in real time.
On the flight up north to be with my family while Pop Pop was hospitalized, I reflected and began to understand some of what was to come — conversations about hospice, fears of the unknown, questions, worries, and sadness — while still needing to maintain a level head for conversations with the healthcare team, patience and compassion when speaking with my family, and appreciation for the quality time I still had with Pop Pop.
When I thought back to my initial concerns for Mom Mom’s care nearly 20 years ago — for her to have respect and dignity until the end of her life, not to be forgotten, ignored, silenced, or disregarded — I began thinking about what that would look like for Pop Pop and his current experience. I slowly started to accept and understand that this was somehow the end of his life. I did not know when that time would come, but I knew it was on the horizon. My family had a direct hand in cultivating a peaceful, comfortable transition surrounded by love, at home rather than in a nursing home like my grandmother. I also felt an immense sense of responsibility to ensure my family had a peaceful experience because they would continue living in the home where Pop Pop would take his last breath. Having to help guide my family through difficult conversations about the care and impending death of our family patriarch was one of the most impactful experiences of my life.
Since I’m not a hospice nurse, I received a crash course through the hospital and hospice staff, a few patients who shared their experiences with me, Google, YouTube, my Drexel education, and good ol’ intuition! As far as in-home hospice care goes, for those wondering, hospice provided eight hours of continuous nursing care to make sure Pop Pop was comfortable and that we had all the supplies and a game plan for his home care. After that, I was largely on my own with on-call support and a daily check-in from the hospice nurse. I should also mention that I was still working remotely with my diabetes patients during the last week of Pop Pop’s hospital stay until he came home on hospice care, where I took over his care. I was honest with my patients throughout this month-long experience, and many of them rode the rollercoaster with me. I occasionally had to reschedule visits or run behind while trying to participate in family meetings or catch doctors when they stopped by Pop Pop’s hospital room. I truly have the best patients and job one could ask for because both were incredibly flexible, understanding, and poured out empathy that still warms my heart.
The night before his passing, my sister and other family members joined my parents and me for dinner at the house with Pop Pop in his hospital bed, surrounded by family and laughter. After spending two days intently monitoring him, I noticed something had changed, so I urged everyone to spend quality time with Pop Pop and give him permission to let go. He later transitioned with my mom and me less than 10 feet away from him. His skin was still warm when I woke up and realized the heavy breathing sounds had stopped in the early hours of Friday the 13th. Much like the birthing process, the dying process can naturally last anywhere from several weeks to just a few hours. In that regard, I was his death doula/hospice nurse. As a nurse passionate about Geriatrics, neither of these professions are new to me, but they have a profound, new living meaning to me. I’m certain hospice and grief support will be revisited in my professional and business endeavors in the form of personal healing, as well as community support and education.
Many of us have loving experiences and memories with our grandparents; I am no exception. My sister and I were the apples of my grandparents’ eyes growing up — she got all the solo attention for five years until I came on the scene to split it! They showered us with love, laughs, and lessons we continue to learn from and smile about. Maaaany summers were spent riding my bikes and walking with Mom Mom, reading and completing book reports, or Pop Pop making cheese sandwiches for my sister and me for a quick lunch. To be involved with both of my grandparents’ care was the biggest thank you I could ever repay them with. As I continue to process Pop Pop’s transition a couple of months ago, as well as my role as both a nurse and granddaughter, I recognize that I had the incredible privilege and honor of caring for two people who supported, loved, and sacrificed so much for our family and me.
Can you talk to us a bit about the challenges and lessons you’ve learned along the way. Looking back would you say it’s been easy or smooth in retrospect?
I transitioned into a Diabetes Nurse Educator role with the new Virtual Diabetes Program while about halfway through grad school. This was a brand-new program that needed to be built from the ground up. My teammate and I had to figure out how to create an education program from scratch, including developing curriculum materials, visual education resources, support tools, and conducting staff and provider trainings.
There are some signs you simply cannot deny as confirmation, and the next part felt like one of mine. Around the time my teammate and I realized everything we had to build, I questioned whether I had bitten off more than I could chew. Lucky me — the next semester of grad school focused on program development, where we learned the process of designing targeted, evidence-based interventions to improve community health. This included assessing population needs, planning activities to address those needs, implementing services, and evaluating outcomes to promote health equity and prevent disease.
I was able to create the diabetes education program for my job while simultaneously learning how to design, facilitate, and sustain a community health program in graduate school. I also completed my internship at the Department of Health in the STD division, where I had the opportunity to evaluate and coordinate sexual health education services and resources for several historically Black colleges and universities across the state.
My teammate and I created an English and Spanish 89-page visual curriculum book, coordinated with multiple departments, and prepared welcome folders for program participants. Creating, implementing, and then actively working within the program while balancing graduate school, recovering from the COVID pandemic, and grieving the unexpected death of a close family member was CHALLENGING. These experiences stretched me professionally and personally, but they also confirmed my ability to lead meaningful community health initiatives. Our program has improved the lives of hundreds of individuals. I learned that I was capable of far more than I initially believed — and later went on to do even more.
About three years into my Diabetes Nurse Educator role, I stepped into nursing entrepreneurship by birthing Prevention is Possible LLC.
Prevention is Possible began as a thought I had at 14 years old when I learned that Alzheimer’s Disease had modifiable risk factors and was not solely caused by genetics. Combining my passions for prevention, education, and advocacy, my business focuses on empowering individuals and communities through holistic education, prevention, and the promotion of generational health and wellness. Although I never initially envisioned myself as an educator, I now recognize that becoming a Nurse Educator has allowed me to build a purpose-driven career while also connecting me to both of my grandmothers, who were educators themselves. My path has always been brightest when collaborating with and educating people.
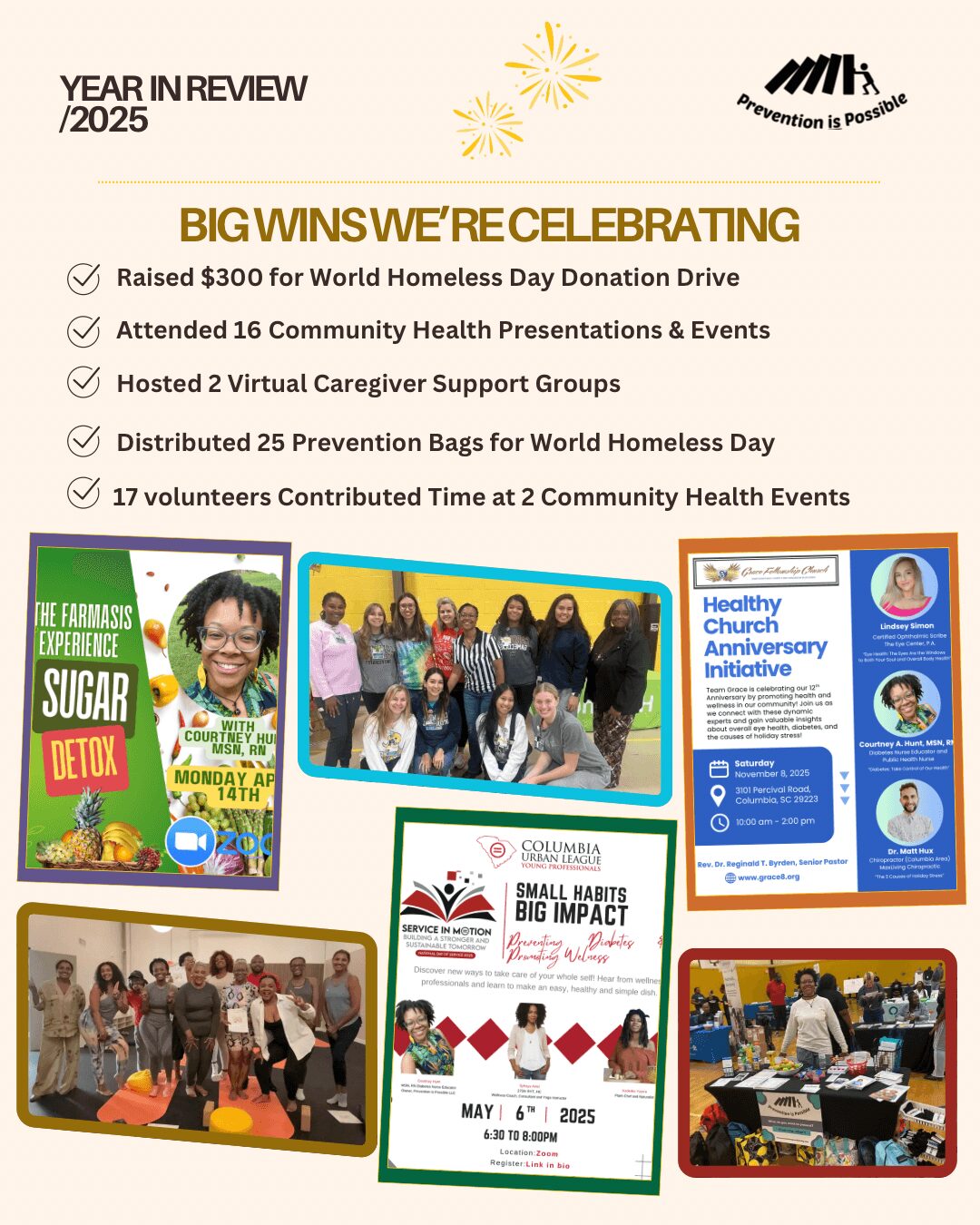
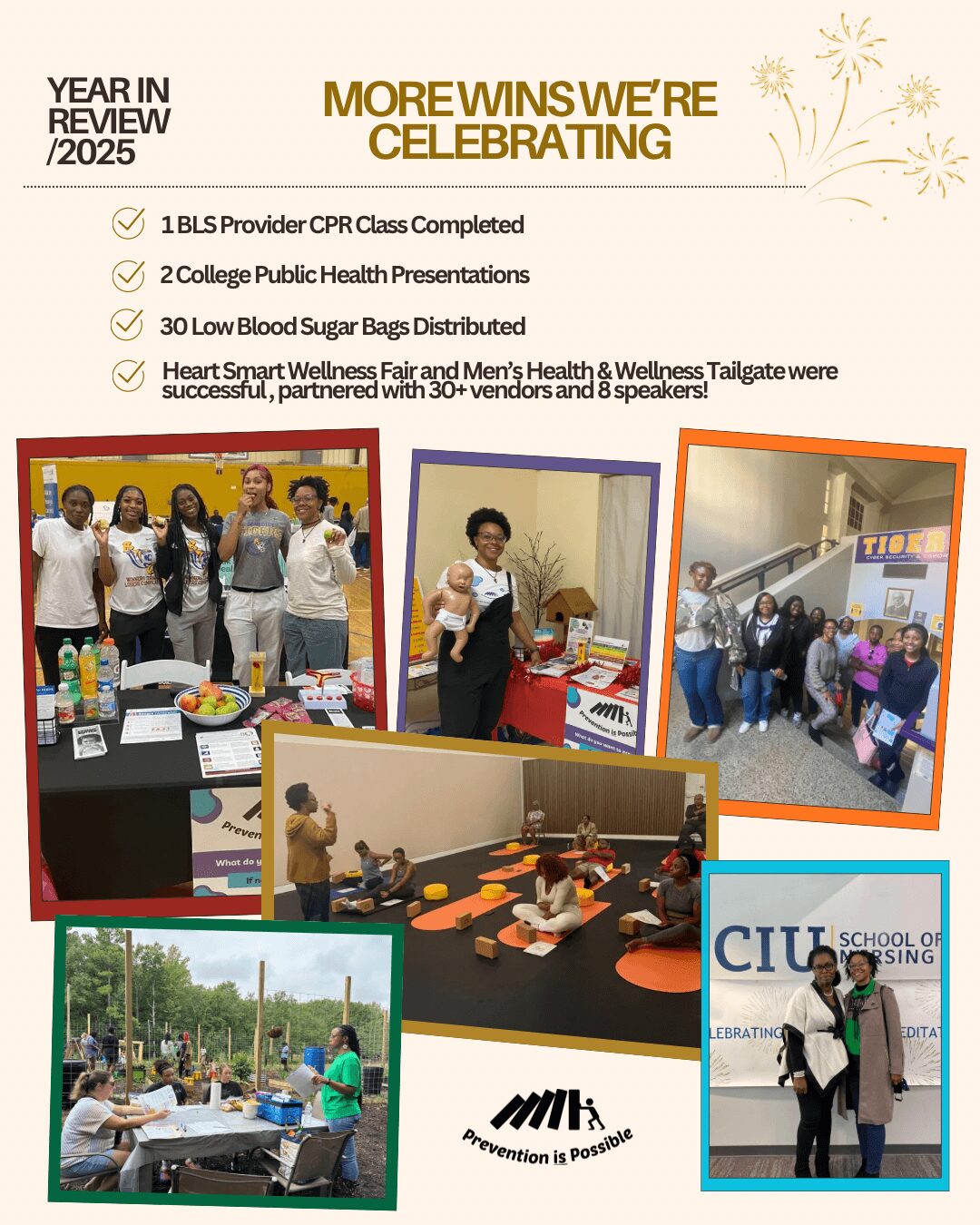
Over the past two years, Prevention is Possible has allowed me to partner with more than 50 local organizations through community presentations, health fairs, donation drives, and college speaking engagements. The work becomes amplified when partnering with others; it is motivating and serves as a reminder that it truly takes a village for all of us to prosper.
As I began learning about nutrition as part of diabetes management, I became curious about where our food comes from and how it is grown, which eventually led me to gardening and farming. After completing a local farming program, Farmasis, I began gardening and quickly fell in love with it. Through gardening, I have learned more about my family’s connection to growing food as well as the many health benefits that gardening provides.
Thanks for sharing that. So, maybe next you can tell us a bit more about your work?
After graduating from Drexel University as a Registered Nurse, I intentionally pursued community-based nursing opportunities rather than hospital nursing. I have an exuberant amount of respect and appreciation for emergency and acute care professionals; however, emergencies are not my comfort zone. I worked in home care, geriatrics, rehabilitation, and preventive care because I have always been drawn toward helping people maintain their health or prevent disease altogether rather than simply treating illness. I love nursing, and to continue this work for the rest of my life, I want it to be in a sector of nursing that I genuinely love and enjoy: community and preventive care.
My career evolved through several community-focused roles, including working with seniors, medically complex children, and underserved populations. I even worked on the Dunkin’ Donuts Community Cruiser and as a bike courier for DoorDash while also working as a companion and home care nurse. Eventually, I found a strong professional foundation at a hospital I swore I would never work at — but I found a loophole! For about three years, I worked at a hospital-based sub-acute rehabilitation and skilled nursing facility, where I gained mentorship, leadership experience, and exposure to quality improvement initiatives. I became a charge nurse and participated in leadership projects through the Magnet committee, where I learned how advocacy and systems-level improvements positively impact patient outcomes. Like every chapter of my nursing career, this role was challenging, balancing the management of both patients and staff, but little did I know it would become a stepping stone for bigger things to come (hint: COVID). A few months after the unexpected passing of a close family member, I relocated to South Carolina. Eager to see what community health looked like in the South, I began searching for non-hospital healthcare roles and eventually found myself at a Federally Qualified Health Center (FQHC) in the Midlands of South Carolina, working as a Nurse Manager at a walk-in health clinic. A few months into my new role in a new state, a new challenge emerged: COVID-19.
When I arrived in the South, I expected to be greeted by “southern hospitality,” especially coming from “The City of Brotherly Love.” However, the pandemic stripped away much of that courtesy and left fear and confusion behind for many of the South Carolinians we encountered each day. Our staff was cursed at, spat upon, yelled at, and endured far more than the fears of the COVID-19 virus itself. Many people were afraid, grieving, and angry with very few outlets. As a healthcare space, we became one of those outlets, and we helped as many people as possible, both physically and mentally, throughout the pandemic. I also cannot move forward without acknowledging the kind words, surprise lunches, and acts of gratitude expressed by many community members, as well as the grit, patience, and commitment to the organization’s mission that our team demonstrated every day.
As terrifying, stressful, disheartening, and relentless as life during COVID was, working in a new state at a walk-in clinic during a global pandemic we had not encountered in roughly 100 years solidified my interest in Public Health Nursing and launched my pursuit of it. It was the first time I directly witnessed the impact of both global health and community health in real time. I began researching how hospitals and healthcare systems in other states and countries were managing COVID, especially during those early days before guidelines were established and before we understood masking and social distancing. Even after those guidelines were introduced, I was responsible for enforcing them among both staff and patients entering the clinic. I monitored inventory based on projected COVID statistics from the public health department while also assessing what we were seeing and using daily in the clinic. At the height of testing, we performed approximately 1,000 COVID tests per month for two to three consecutive months. The days were long, the work was constant, and chest palpitations were not uncommon for me during that time.
During the pandemic, a close high school friend passed away after contracting COVID, and I was unable to attend his funeral back home because of work demands and concerns about my own daily exposure. We frequently saw positive cases after people attended funerals or other large gatherings. Looking back, all of my previous community-based experiences prepared me for COVID: working on the Community Cruiser, serving coffee to hundreds of demanding people, enduring verbal bullying from previous nursing supervisors, maintaining order and enforcing workplace policies as a nurse manager, and critically thinking through problems in home care settings with minimal in-person support.
As the peak of COVID declined, I decided to return to school for my Master’s Degree in Nursing with a concentration in Public Health. I felt like a kid in a candy store (nerd alert!) — I loved graduate school. I was finally putting everything together: nursing, community, and prevention equaled public health nursing. About halfway through my master’s program, I began feeling bored at work after being introduced to so many new public health concepts and ideas. When my director asked what I was interested in pursuing, it suddenly came to me: prevention. I was later offered a diabetes nurse educator role with a newly developing program. Up until that point in my nursing career, I had never considered diabetes care, management, or prevention, but it truly became the next stepping stone toward my purpose. Graduate school helped me connect nursing, prevention, and community health into a clear vision for my future work.
If we knew you growing up, how would we have described you?
My nursing roots and interests in geriatrics, prevention, and advocacy stem from caring for my grandmother with Alzheimer’s Disease as a teenager. Caregiving for others comes naturally to me because of the close relationship I shared with my grandmother; she will always be my first patient who taught me about patience, empathy, and other qualities important for caregiving.
As a teenager, I became deeply interested in chronic disease prevention and lifestyle habits. I began recognizing patterns within my own family and understanding how stress, behavior, and access to care influence long-term health outcomes. Those realizations and evidence-based research planted the seeds for my passion for prevention and public health. After learning more about the trajectory of Alzheimer’s Disease, I shifted away from physical therapy and chose nursing around the tenth grade.
When my grandmother’s care at home became unsafe for both her and my grandfather. One defining moment is when she wandered out of the house, and the family had to search for a few hours until they found her, sitting at my elementary school playground a few miles from her home. She later moved into a nursing home (also known as long-term care, LTC) with 24/7 nursing care and monitoring. My grandfather visited daily, while the rest of our family visited multiple times throughout the week, at all hours of the day. Within a few months, we had built relationships with residents whose families were unable or unwilling to be present, including my grandmother’s roommate, Cherrie, who had never married or had children and had no one to care for her in her golden years.
Mom Mom’s LTC experience and my professional experience working at an LTC have shown me that long-term care facilities are not inherently bad and do serve a necessary purpose, especially as people are living longer; they are, however, often under-resourced and poorly managed. It also inspired my long-term goal of adding a long-term care administrator to my resume, as geriatrics will always hold a special place in my heart. Supporting my grandmother through Alzheimer’s Disease shaped the way I viewed health, aging, and family responsibility from an early age. I quickly learned that health challenges affect entire families, not just individuals. I volunteered with the Alzheimer’s Association since high school, throughout college, and still share their services to patients and community members. I saw the power of volunteerism and advocacy, and participated in National Day on the Hill, where our local chapter spoke to state representatives at the U.S. Capitol. I saw how Alzheimer’s knows no limits and touches all races/ethnicities and economic statuses when my mom and I would volunteer annually at the Walk to End Alzheimer’s – family and friends would join us from out of town. The love I have for my patients and the work I do comes directly from my experiences as a caregiver and from witnessing how chronic illness impacts families as a whole.
Pricing:
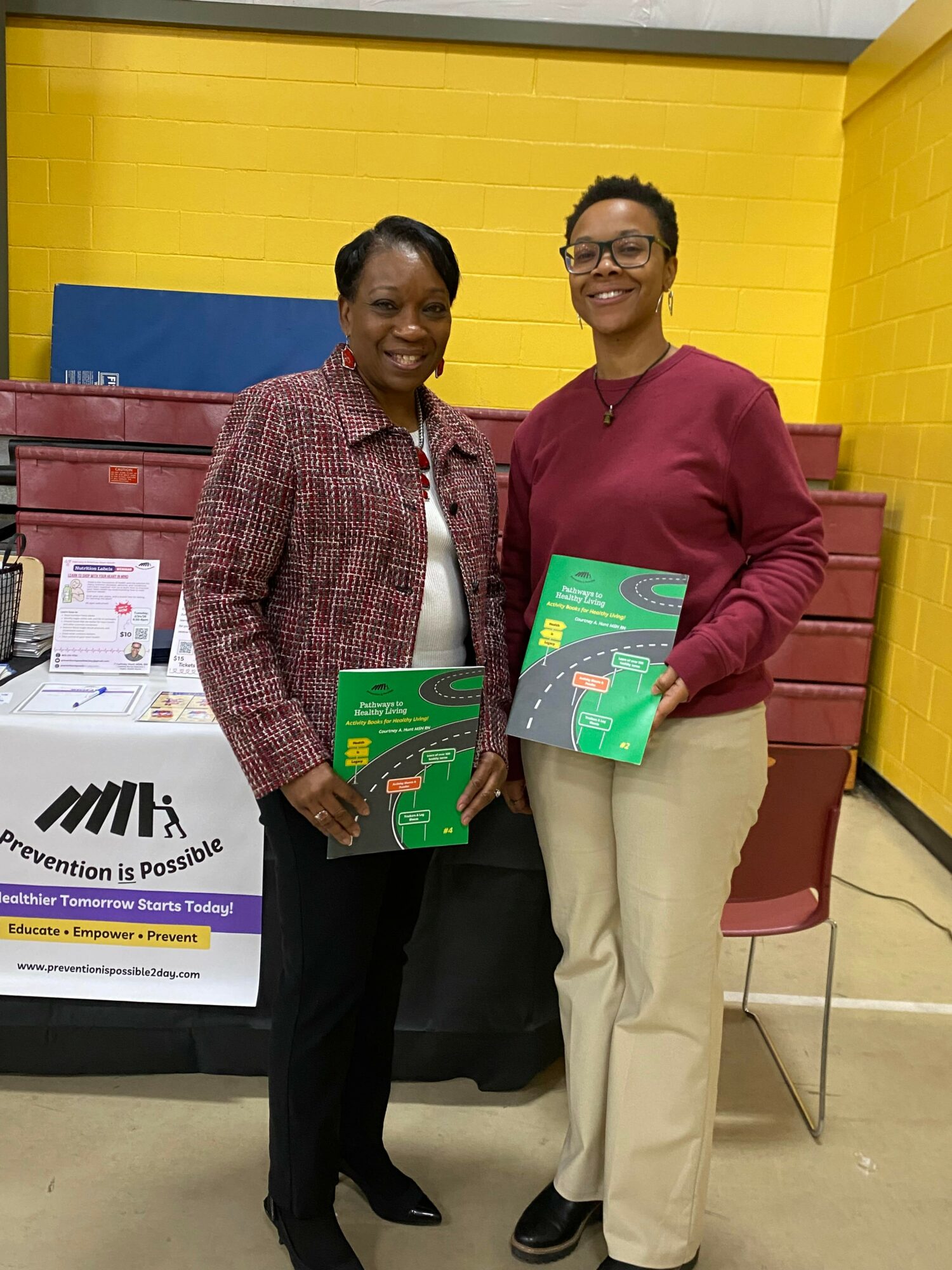
- Pathways to Healthy Living Activity Books – $10 to $20
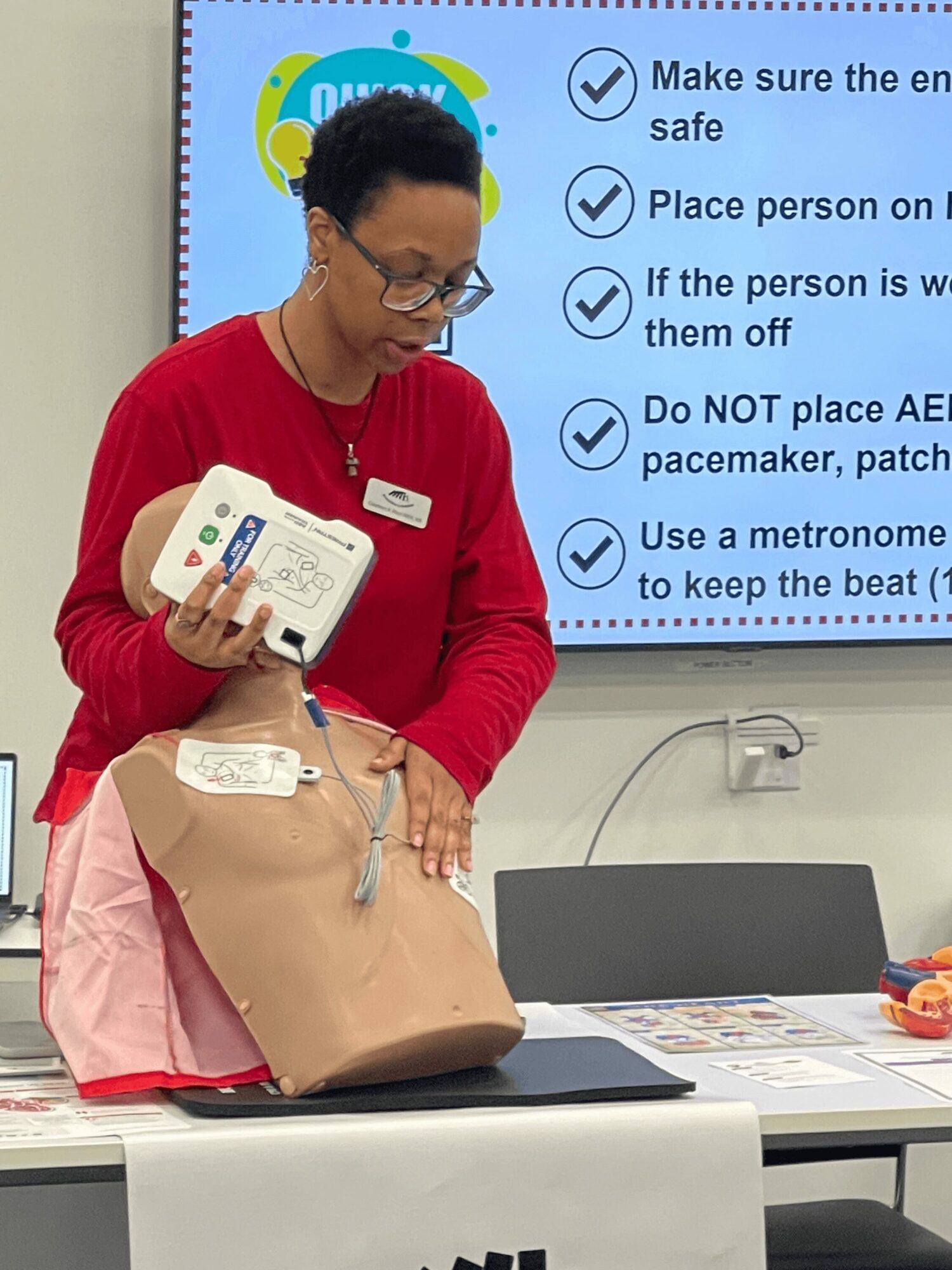
- CPR Courses (Heartsaver / BLS) – In Person ONLY – $75 to $100
- 2 hr Group Presentations – $150
- Check Your Self Mug – $14
Contact Info:
- Website: https://www.preventionispossible2day.com/
- Instagram: https://www.instagram.com/preventionispossible_2day/#
- Facebook: https://www.facebook.com/profile.php?id=61575254810815
- Other: https://linktr.ee/preventionispossible2day